
 Human movement is dependant upon precise limb/trunk coordination.
Human movement is dependant upon precise limb/trunk coordination.
Due to the lack of a sufficient intrinsic structural stability of the trunk – most notably in the spine itself – children with special needs lack the spinal strength and mobility necessary for initiating movements from the trunk.
The stiff or immobile spine leads to disrupted limb to trunk coordination, which becomes obvious both when the children attempt to move or when movements are initiated with them from without.
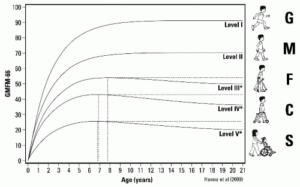
The inhibitions in the sequence of movement between trunk and limbs in a child with special needs leads to the various difficulties the children experience when trying to carry out movement sequences and weight bearing functions. When the child is small it is often possible to attain a functional level through training and exercising, but this level often diminishes when the child grows and the limb trunk proportions change through normal growth. This deterioration in function is evident in the GMFCS motor score curves seen clearly with the GMFCS Levels III, IV, and V:
Typical of this lack of a sufficient trunk limb coordination is also a tendency to carry out “robotic” movements, to use excessive muscular effort and also to require a high level of concentration for carrying out movements.
Older and adult individuals on the other hand may have developed some level of gross motor function, but this function can also most frequently be characterized as ”stereotype” or ”robotic” in nature. This robotic function often leads to joint distortions, stiffness, pains and discomforts, etc.
The purpose of ABR exercises is to create the environment and the conditions that support the child or adult to develop and to initiate the undulatory motions of the spine rquired for creating the proper trunk limb coordination. ABR applications achieve this at ages and stages where it is normally no longer possible for the person to establish this coordination themselves. In fact the integration of these primary movements and stages of movements connected to the spine, belong to the earliest motor developmental moments of life – which normally are completed between birth and six months of age. If this coordination is not already established by then, the child or adult can no longer initiate and establish these intrinsic movements on his own.
ABR Techniques open a new door of opportunity for such individuals.
The sequences of activation necessary relate not only to the trunk and the limbs in their related coordination, but also correspond to specific muscle fiber types belonging to the trunk and limbs respectively.
The muscle fiber types that react first during normal muscular activation are most highly integrated within the trunk (type one) and those that have a higher reaction threshold (type two) are more highly integrated within the superficial muscle layers of the limbs.
Whe persons with Cerebral Palsy, or other illnesses affecting the motor skill function go through training or ordinary rehabilitation and other exercises – this out of necessity will tend to initiate an inverted sequence of reaction within this highly organized muscle reaction sequence.
The waking up of and activation of the type one muscle fibers of the trunk belongs intrinsically to ABR work which is designed to install the “baby stages” of deep intrinsic undulatory spine movement in children and adults who have long left the baby age – and also in those children who may be at this young age and are too weak or too stiff to initiate the proper coordination between the deep intrinsic muscles of the trunk and those of the limbs on their own.
ABR Techniques for the spine and trunk are based upon a re-integration of a proper trunk-limb coordinatinon. To further support the active integration of these movements we have a variety of specialised techniques:
ABR based active exercises that we call PAVES or “Peri-Articular Visco-Elastic Stimulation”. These exercises work to strengthen the trunk, encourage the development of deep undulatory trunk movement, stabilize the joints, etc. without causing stress to the persons weak structures and without creating a high cost to the individual’s energy household level. These exercises involve the application of specific and well-controlled movements applied : soft gymnastic balls, soft room trampolines and visco elastic pillows and materials.
TheraTogs Usage is in itself a great way to promote a healthy coordination of limbs and trunk. The TheraTogs is a specialized garment that helps children with special needs to stabilize their trunk. When trunk stability is present and the child is not so highly dependant upon muscle tension for creating this stability, then the trunk can react in a more appropriate manner and it is possible to establish the proper sequence of activation of the limbs in respect to the trunk. This garment can easily be integrated into daily routines. It will add a significant advantage to all movements performed by the users. It adds tensional uniformity and intrinsic pre-stress to the trunk , which in turn allows for a higher freedom of limb activation. At the same time it encourages physiologically sound tissue remodelling – creating a continuously improved intrinsic foundation for movement development.
Diane Vincentz
Director
ABR Denmark Aps

