Children with special needs will all in some manner be affected with what is termed “Global Developmental Delay”. This indicates that the entire development of the child is affected to such a degree that all the defined major developmental areas (officially at least two of the areas) are affected, specifically:
- Motor development
- Speech and communication
- Cognitive
- Social and emotional development
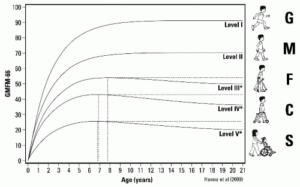
In reality however these developmental areas are not disconnected and disengaged from each other. In any organism, and in the human being at a much higher level, all of these different developmental areas are highly intertwined and decidedly connected. In fact, as our developmental hierarchy graph below attempts to illustrate, the different areas of development are not only interwoven with each other, but the developmental potential of the so called “higher and cognitive levels” is dependant upon what happens at more basic and fundamental levels.

One example that illustrates the difficulty in attempting to disconnect the developmental areas from each other can be understood when one observes human speech and communication development.
Within the world of the Speech Therapy specialists it is known and widely accepted that a child who cannot adequately swallow and chew will not be able to learn to speak. This shows us how in the human being so called “higher functions” such as speaking are dependent upon at least a minimal level of basic life functions. In effect it is so that if a child cannot chew and cannot swallow, and – in addition – has a sufficient weakness of the respiratory level, then any attempts to “teach” the child to speak with speech intervention methods will be in vain.
This does not mean that the child cannot learn to communicate, use a computer-based program or learn some basic skills in this fashion. But, speech as a skill involving our entire speech organism, will normally be closed for the child due to the fact that the human speech is dependant upon a finely tuned motor coordination between:
- The respiration – coordination of the air flow through the larynx and trachea
- Epiglottis as articulator
- Pharyngeal coordination
- Mouth floor control
- Tongue
- Hard and soft palate coordination
- Mimic muscles of the face
- Lips
- Jaw
- Sinuses and skull as resonators, etc.
The list of the structures that need to be fine tuned and well coordinated for speech function is long and exceedingly complex. Yet a healthy child between the ages of 0- 3 years – through an intense ability to imitate the activities of the people close around him – begins to utilize these structures and to coordinate them in a highly complex fashion in order to be able to use speech as a means of both emotional and later intellectual communication.
A child who suffers from Global Developmental Delays will have difficulties related to all four of the main accepted developmental areas. There is almost nothing in his or her own development that will not be touched. From the side of the rehabilitation it would make sense if the child could be sent to a Global Developmental Specialist. But this profession does not exist. The typical result for the child and family is then that the child will be dutifully sent from one specialist to the next:
- The speech therapist
- The occupational therapist
- Riding therapist
- Swim therapy
- Eye Doctor
- Neurologist
- Orthopedic specialist
- Physio-therapist
- Special Education teacher
And the list goes on and on.
ABR Program and Method has shown that for children especially, all development is “Global”. One cannot disconnect one area of development from the other – in the human organism development of one “area” is dependant upon the stability of other areas. We cannot dissect the developmental regions and place them on the floor of some workshop as one can do with a car – put the brakes in one corner, the carburettor here, the engine there, the starter motor on another spot! This does not work with the human being. Activities and capabilities rest upon each other – are interdependent and co-exist.
The parents and children in the ABR Program have found a fortunate means of global developmental enhancement. ABR is a Program that promotes transformation of all developmental levels respecting the inter-connectivity of processes within the human being.
If as an ABR Parent one comes to work on the neck or the throat of the child one will be promoting a wide variety of functions all at one time. ABR neck applications typically help the child with:
- Stability of the upper respiratory tract – improving respiration flow
- Swallowing
- Neck stability
- Head control
- Eye stability – even vision
- Sound production and variation of tone
- Inner coherence of the proprioception – body map
- Connectivity in respect to the surroundings and environment
In this way we can see that the soft tissue remodelling achieved through ABR applications work as a foundation for the child’s higher development – whether having to do with basic life functions which are depnedent upon a stable intrinsic strength of connective tissues, – or higher capabilities such as speech and understanding.
ABR works as a Global Developmental Enhancement tool, allowing parents and caretakers to dramatically change the life and life quality of mild to severe handicapped and special needs children.
Diane Vincentz
ABR Denmark
Director
 Human movement is dependant upon precise limb/trunk coordination.
Human movement is dependant upon precise limb/trunk coordination.